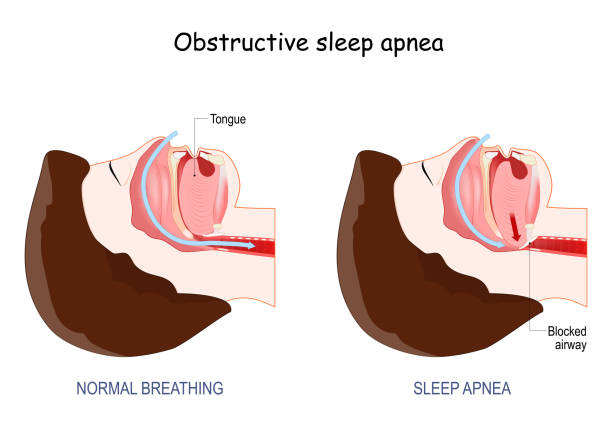
Sleep apnea is a sleep disorder that can be divided into two categories: obstructive sleep apnea and central sleep apnea. People with sleep apnea can experience daytime sleepiness, and if left untreated, can lead to sudden death. To avoid this, treating sleep apnea with continuous positive airway pressure (CPAP) is essential.
Depending on the severity, sleep specialists may recommend mild, moderate, or severe sleep apnea treatment. A sleep study is often required to determine the best approach for treating sleep apnea. If you or a loved one has been diagnosed with sleep apnea, it is important to consult with a sleep specialist to understand the signs, symptoms, and consequences of untreated sleep apnea.
Is Sleep Apnea Dangerous?
Sleep apnea is a disorder that causes breathing to temporarily stop or become restricted during sleep. People with this condition can experience severe health problems, such as diabetes, stroke, heart failure, cognitive impairment, and even death. Obstructive and central sleep apnea are the two main types.
Sleep Apnea Solutions & Treatment can include CPAP (Continuous Positive Airway Pressure) and other therapies prescribed by a sleep specialist. Obstructive Sleep Apnea Syndrome (OSAS) is a severe form, while moderate and mild forms exist. A sleep study may be required to diagnose the disorder and determine the best treatment.

What Are the Risks of Untreated Sleep Apnea?
Sleep apnea is a disorder that is usually caused by obstruction or the inability to initiate breathing. Obstructive sleep apnea is the most common type and can lead to serious health issues if not treated. Central sleep apnea is less common and is when the body can’t initiate breathing.
Treating sleep apnea with CPAP (Continuous Positive Airway Pressure) can help people with mild, moderate, or severe obstructive sleep apnea. A sleep specialist may recommend a sleep study to diagnose sleep apnea and determine the best treatment. People with sleep apnea may experience daytime sleepiness.
- High blood pressure: Obstructive Sleep Apnea is a sleep disorder that can cause loud snoring, pauses in breathing, and low oxygen levels. It is a risk factor for high blood pressure and can be treated with Positive Airway Pressure. Untreated Sleep Apnea can lead to developing more severe forms such as Treatment Emergent Central Sleep Apnea and Undiagnosed Sleep Apnea. People can fall asleep more easily when Sleep Apnea is diagnosed and treated.
- Diabetes and insulin resistance: People with mild obstructive sleep apnea may fall asleep easily, but are at risk for developing sleep-disordered breathing. Untreated sleep apnea may lead to loud snoring and can cause the patient to stop breathing at night. This can lead to an increased risk of developing diabetes due to insulin resistance. Positive airway pressure and other treatments can help diagnose and treat sleep apnea, helping to lower blood pressure and reduce risk factors.
- Pulmonary hypertension: Sleep apnea is a sleep disorder in which a person can stop breathing while asleep. Loud snoring and falling asleep during the day are risk factors for sleep apnea. Obstructive sleep apnea is the most common type and is caused by air pressure in the throat collapsing during sleep. If left untreated, sleep apnea can lead to high blood pressure and other health problems.
Treatment for sleep apnea includes positive airway pressure and emergent central sleep apnea. Diagnosing and treating sleep apnea may help to reduce the risk of developing pulmonary hypertension, a condition in which the blood vessels in the lungs have changed due to breathing disruptions.
- Stroke: Healthy sleep is important for maintaining good oxygen levels in the blood. Obstructive Sleep Apnea (OSA) is a common condition that can cause high blood pressure and other health issues. Treatment with oral appliances, sleeping pills, and clinical sleep medicine can help prevent OSA.
How is sleep affected by losing weight, falling asleep, and upper airway resistance? Daytime fatigue, nonalcoholic fatty liver disease, and other chronic lung diseases can be caused or worsened by OSA. Treating OSA with bilevel-positive airway pressure and central sleep apnea can help prevent stroke.
- Abnormal heart rhythms: Sleep apnea happens when a person’s upper airway is blocked, preventing them from getting enough oxygen during sleep. This can lead to abnormal heart rhythms, also known as arrhythmias, which may be a cause of sudden death in those with sleep apnea. Clinical sleep medicine and healthy sleep practices, such as nonalcoholic fatty liver disease and losing weight, can help prevent sleep apnea. Other treatments such as oral appliances, bilevel-positive airway pressure, and sleeping pills can also help. Oxygen levels, high blood pressure, and daytime fatigue are common in those with sleep apnea. Central sleep apnea (CSA) and obstructive sleep apnea (OSA) are two different types of sleep apnea. How is sleep can be improved by treating sleep apnea and preventing it from happening.
Obstructive Sleep Apnea (OSA) is a condition where the upper airway is blocked, reducing blood oxygen levels and leading to daytime fatigue and other problems. Treatment options include oral appliances, sleeping pills, losing weight, and Bilevel Positive Airway Pressure.
Clinical Sleep Medicine is important to assess how is sleep and prevent OSA, as it can increase blood pressure, impair memory and worsen mood, and increase the risk of accidents. Central Sleep Apnea (CSA) and Nonalcoholic Fatty Liver Disease can also occur due to untreated OSA. Healthy sleep is essential for the body to function properly.
Can Sleep Apnea Cause Death Suddenly During Sleep?
People with sleep apnea have an increased risk of sudden cardiac death. Treatments like oral appliances, airway pressure devices, and weight loss can reduce this risk. Sleep apnoea is caused by a narrowed airway and weak upper airway muscles. This can lead to restless sleep, loud snoring, and trouble concentrating.
Other sleep disorders, like emergent central sleep apnea, can lead to breathing and oxygen levels dropping during sleep. Soft palate and throat muscles also play a role in causing metabolic syndrome and atrial fibrillation. Treating these conditions with devices and lifestyle changes can help people achieve normal sleep and reduce their risk of complications.
Signs of Sleep Apnea
Sleep apnoea is a disorder where breathing and oxygen levels during sleep are disrupted. It can be identified by snoring loudly and gasping for air. Other signs include trouble concentrating, restless sleep, and increased risk of metabolic syndrome, atrial fibrillation, and other sleep disorders. Narrowed airway and upper airway muscles, along with a soft palate, can cause sleep apnoea. Weight loss and airway pressure devices, such as oral appliances and other airway pressure devices, can help to restore normal sleep. This can reduce the risk of emergent central sleep apnea.
Additional signs and symptoms of obstructive sleep apnea include:
- Waking up gasping for air or choking
- Making unusual sounds while sleeping
- Having frequent daytime fatigue
- Waking up unrefreshed
- Falling asleep during daytime tasks
- Experiencing morning headaches
- Tossing and turning during sleep
- Having mood swings
- Difficulty concentration during the day
- Urinating frequently during the night
People with central sleep apnea may have similar signs and symptoms of obstructive sleep apnea. These may include snoring loudly, restless sleep, trouble concentrating, daytime sleepiness, and weight loss. Other symptoms are lower oxygen levels and decreased breathing.
Treatment may involve the use of an oral appliance, other airway pressure devices, weight loss, and exercise for the upper airway muscles. Emergent central sleep apnea can cause atrial fibrillation and metabolic syndrome, which can increase the risk for other sleep disorders.
When to See a Doctor
People with sleep apnea may experience symptoms such as daytime sleepiness or not feeling rested in the morning. Sleep specialists can diagnose sleep apnea with a sleep study. This test monitors brain signals and records changes in heart rate and breathing. Sleep apnea can be mild, moderate, or severe. Treatments can include continuous positive airway pressure (CPAP) and other therapies. Prompt treatment can help prevent complications.